中国组织工程研究 ›› 2014, Vol. 18 ›› Issue (53): 8641-8645.doi: 10.3969/j.issn.2095-4344.2014.53.021
• 骨与关节生物力学 bone and joint biomechanics • 上一篇 下一篇
单节段减压融合内固定修复多节段腰椎间盘突出症合并腰椎滑脱:改善支撑力及应力的动态平衡
王晓平,马华松,陈志明,袁 伟,秦柳花,任冬云,郑 蕊,张 敬,辛 莘,陆 明
- 解放军306医院骨科,北京市 100101
Single segmental decompression and fusion for repair of multi-segmental lumbar disc herniation with lumbar spondylolisthesis: improvement in dynamic equilibrium of supporting force and stress
Wang Xiao-ping, Ma Hua-song, Chen Zhi-ming, Yuan Wei, Qin Liu-hua, Ren Dong-yun, Zheng Rui, Zhang Jing, Xin Xin, Lu Ming
- Department of Orthopedics, the 306 Hospital of Chinese PLA, Beijing 100101, China
摘要:
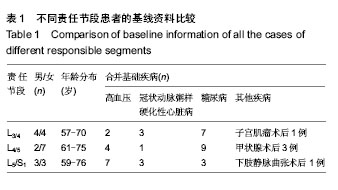
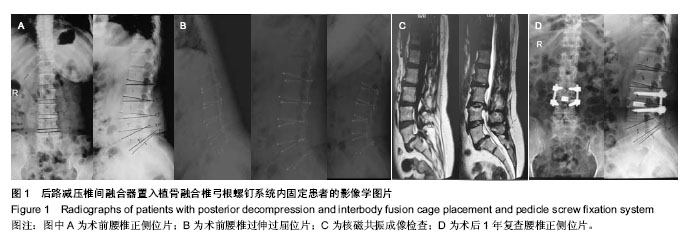
背景:腰椎退变性疾病多见于老年人,因此导致手术风险居高不下。为了解决这一问题,部分学者提出了选择性减压的概念,但对于部分患者仍然难以明确责任节段或部位,从而导致在多项前瞻性的随机对照研究中选择性减压技术并未能较广泛性减压获得更好的修复效果。 目的:分析腰椎退变性疾病中多节段腰椎间盘突出症合并腰椎滑脱患者单节段减压融合内固定修复的有效性。 方法:选择2010年1月至2013年12月收治的多节段腰椎间盘突出症合并腰椎滑脱患者23例。修复方法主要为单节段减压融合内固定,采用常规X射线、腰椎MRI 检查结合选择性神经根封闭,以及动态X射线测量(过伸过屈位及左右侧屈位)等判定病变阶段及不稳定区间。经动态X射线测量采用Posner评分明确责任节段稳定性;经腰椎MRI确定椎间盘明显退变变性;选择性神经根封闭,明确主要责任间隙。采用腰腿痛目测类比评分、日本骨科协会评分对患者的修复效果进行评定,加用临床症状改善程度作为疗效的判定标准。 结果与结论:患者均获得12-36个月随访,末次随访患者腰腿痛目测类比评分、日本骨科协会评分均较术前明显改善,末次随访日本骨科协会评分改善率为88%,目测类比评分改善率为93%。未见术后出现神经根刺激症状的病例,所有患者均获得融合节段的骨性融合,无内固定无松动、断裂和拔出现象,无腰椎矢状位失平衡。提示多节段腰椎退变伴邻近节段腰椎滑脱患者,在术前根据症状体征和影像学特点给予正确、全面诊断、评估,对病变责任间隙予以减压、采用短节段内固定治疗,椎弓根钉和连接棒以及椎间植骨融合可增加前中柱的支撑力,使内固定钉棒上的应力维持动态平衡,同时稳定的钉棒内固定系统也有利于前方植骨材料的骨愈合。内固定器械形成的框架式结构,使其抗旋转能力显著提高,从而形成坚强的三维固定。
中图分类号: